

Most massage therapists think SOAP notes are just annoying paperwork until a state board investigator shows up asking for three years of client records. That's when a simple filing system becomes the difference between staying in business or losing your license.
A wellness center in Portland got demolished during an audit last year. They had 1,800 active clients, seven therapists, and what looked like a successful operation pulling around $45k monthly. The owner kept client notes in a combination of paper folders, therapist notebooks, and a shared Google Drive. When the state board requested documentation for a specific client complaint from 18 months prior, they couldn't produce complete records. The therapist who handled that client had left six months earlier and took her personal notebook with her.
The audit expanded. More missing notes surfaced. Insurance claims from two years back had no supporting documentation. The state found they'd been billing for 60-minute sessions but only had intake forms, no actual treatment records. Final damage: $28,000 in fines, suspended insurance billing privileges, and one therapist lost her license. The business closed four months later.
This wasn't about lazy record-keeping. The owner genuinely thought she had a system. She just never understood that SOAP notes aren't really about documenting treatments—they're about creating a legally defensible operational structure that protects your entire business.
Why SOAP documentation breaks down in real wellness practices
The typical massage therapy business starts with one or two therapists who keep notes however feels natural. Maybe you write detailed narratives about each session. Maybe you use a basic form you downloaded online. Everything seems fine when you're seeing 15 clients a week.
Then growth happens. You hire another therapist. Now you've got two different note-taking styles. You add chair massage for corporate clients—different documentation needs. You start accepting insurance—suddenly you need specific codes and treatment justifications. You bring on a part-time therapist who only works weekends—their notes live in a separate system.
By the time you hit 100+ weekly appointments across multiple therapists, your documentation system has become a patchwork of different formats, storage locations, and retention practices.
The original therapist writes novels. The new hire uses bullet points. One keeps digital notes on their tablet. Another prefers paper forms. Nobody follows the same template. Documentation drift happens fast. Each therapist gradually develops their own shorthand and format. What starts as minor variations becomes completely different documentation styles.
Try reading notes from three different therapists about the same client—they might as well be writing about different people.
Retention becomes chaos too. Some notes get filed immediately. Others sit on desks for days. Digital notes live in personal folders. Paper notes pile up waiting to be scanned. When someone quits, their documentation system leaves with them. You end up with gaps that only become obvious during an audit.
Handoff failures are brutal. When clients see different therapists, critical information gets lost. The Tuesday therapist doesn't know about the shoulder issue the Saturday therapist has been addressing for three weeks. Clients get frustrated repeating their history. Treatment continuity breaks down.
Billing disconnects cost real money. Your SOAP notes say one thing, your billing records say another. Insurance companies reject claims because documentation doesn't support the billed services. You can't prove medical necessity. Revenue takes a hit while you scramble to reconstruct session notes from memory.
A massage practice in Denver showed me their "system" last month—five different note formats across six therapists, paper forms mixed with iPad notes, no consistent retention schedule, and billing codes that barely matched treatment documentation. They'd been operating this way for three years without major issues. Then a client filed an insurance complaint about treatments from 14 months ago. They couldn't produce matching records between their notes and billing. The insurance company demanded $11,000 in refunds.
The hidden compliance requirements nobody tells you about
Most wellness practitioners learn about SOAP notes in school—Subjective, Objective, Assessment, Plan. Simple enough. What they don't teach you is the web of compliance requirements that determine whether those notes actually protect your business.
Never miss a booking or double-book again.
Masthera helps you schedule, confirm & manage every massage session with ease.
- Unified appointment management
- Automated client reminders
- Therapist calendar coordination
No credit card required
State boards have specific documentation requirements that vary by location but generally include: treatment dates and duration, areas worked, techniques used, client response, contraindications noted, and treatment modifications. Miss any element consistently and you're non-compliant.
Insurance companies layer on additional requirements. They want treatment codes, medical necessity justifications, progress measurements, and objective findings. Your SOAP notes need to support every billing code you submit. Bill for neuromuscular therapy but your notes only mention "general massage"? Claim denied.
Then there's HIPAA. Those client notes are protected health information. Storing them in a therapist's personal Google Drive? Violation. Letting staff take notebooks home? Violation. No encryption on digital files? Violation. Each violation can cost up to $50,000.
Professional liability insurance adds another layer. If a client claims injury, your notes become evidence. Incomplete documentation means your insurance might not cover you. Policies specifically exclude coverage when proper treatment records don't exist.
The retention requirements create operational nightmares. Most states require keeping adult client records for 3-7 years. Minor client records need retention until they turn 18, plus the standard period. Some insurance contracts require 10-year retention. Paper records need secure physical storage. Digital records need backup systems and access controls.
A wellness center in Austin thought they had this figured out—detailed SOAP notes, locked filing cabinets, everything by the book. Then their office flooded. Three years of paper records destroyed. No digital backups. Insurance claims going back two years couldn't be verified. They lost $34,000 in insurance reimbursements and faced state board sanctions for inability to produce required documentation.
Building a legally defensible SOAP system
Creating a SOAP notes system that actually protects your business requires thinking beyond individual session documentation. You need an operational structure that handles creation, storage, retention, and access across your entire practice.
Start with format standardization. Every therapist needs to use the same SOAP template—not similar, identical. This isn't about stifling creativity; it's about ensuring any therapist can read any note and understand exactly what happened in that session.
The template should force completion of every required element. No skipping sections because they seem redundant.
Your SOAP template needs specific fields for: Subjective section: Client's reported symptoms, pain levels (numeric scale), activities affecting condition, response to previous treatment, and current medications or health changes. Objective section: Observable findings, palpation results, range of motion measurements, areas treated with specific techniques, pressure used, and client's observable response during treatment. Assessment section: Progress since last session, effectiveness of current treatment approach, contraindications observed, and professional assessment of condition changes. Plan section: Recommended frequency, suggested home care, referrals made, next session focus, and specific techniques planned.
Aim for 5-7 minutes per SOAP note when designing your template so therapists can complete notes between clients.
Each section needs enough detail to recreate the session two years later but not so much that therapists spend 20 minutes writing notes between clients. The sweet spot is usually 5-7 minutes per SOAP note when using a proper template.
Documentation elements break down like this:
| Documentation Element | Legal Requirement | Insurance Requirement | Operational Need |
|---|---|---|---|
| Session date/time | Yes - all states | Yes - claims processing | Yes - scheduling |
| Areas treated | Yes - most states | Yes - billing codes | Yes - continuity |
| Techniques used | Yes - scope of practice | Yes - medical necessity | Yes - treatment planning |
| Client response | Recommended | Yes - progress notes | Yes - safety |
| Treatment modifications | Yes - standard of care | Sometimes | Yes - risk management |
| Session duration | Yes - billing accuracy | Yes - claims | Yes - scheduling |
| Therapist signature | Yes - authentication | Yes - provider verification | Yes - accountability |
Storage architecture matters more than most practices realize. You need three levels of access: active files (current clients), archived files (inactive but within retention period), and disposed files (documented destruction after retention expires). Each level needs different security and access protocols.
Digital storage requires encryption at rest and in transit. That means encrypted hard drives and secure transmission methods. Email isn't secure transmission—even with passwords. Cloud storage needs HIPAA-compliant vendors with signed Business Associate Agreements. Your cousin's IT company probably doesn't qualify.
Physical storage needs locked cabinets in a secure location. Not the reception desk drawer. Not the break room filing cabinet. A dedicated, locked storage area with limited access. Humidity control matters—moldy records are useless records.
Creating retention schedules that actually work
Retention schedules sound simple until you're managing 2,000 client files across seven years of requirements. The complexity multiplies when different regulations apply to different record types.
Build your retention schedule around the longest requirement that applies. If state law says five years but insurance contracts require seven, keep everything seven years. Simple rule prevents expensive mistakes.
Your retention schedule needs clear triggers:
Start date: When does retention begin? Last treatment date, not first. Client seen weekly for two years then stops? Retention starts when they stop, not when they started. Review date: Annual review to identify records ready for disposal. Mark this in your calendar like tax deadlines. Disposal date: When records hit retention limit, they need secure disposal. Shredding for paper, certified digital destruction for electronic. Document the destruction—date, method, and who performed it.
The real challenge is tracking retention across different storage methods. Paper files from 2019, digital files from 2020 onward, and that weird transition period where you had both. Each needs tracking within your retention system.
A practice in Sacramento learned this the hard way. They switched from paper to digital in 2018. Thought they'd properly transferred everything. During a 2023 audit, they discovered gaps—several months of 2018 records existed in neither system. The transfer process had failed to capture notes during the transition period. Those missing records cost them $16,000 in insurance recoupments.
Handoff protocols and treatment continuity
When multiple therapists treat the same client, SOAP notes become critical coordination tools. But only if therapists actually read previous notes and know how to use them for treatment planning.
Most practices fail here. Therapists grab the client file, flip to a blank page, and start fresh. Previous treatment information stays buried in earlier notes. The client explains their issues again. Treatment starts from zero each time.
Effective handoff protocols require:
-
Pre-session review
Therapists must read the last 2-3 SOAP notes before the client arrives. Not during intake. Not while the client's on the table. Before they walk in.
-
Continuity markers
Your SOAP template needs a specific field for "continuing treatment from [date/therapist]" to create clear connection between sessions.
-
Critical flags
Certain information needs prominence—injuries, contraindications, triggering techniques, emotional responses. These can't be buried in paragraph text.
-
Progress tracking
Objective measurements that multiple therapists can replicate. "Shoulder feels better" means nothing. "Shoulder flexion increased from 110 to 135 degrees" means everything.
One practice I worked with color-coded their SOAP notes by urgency. Red tabs for active injuries, yellow for chronic conditions being treated, green for maintenance care. Any therapist could immediately identify what needed attention. Their client satisfaction scores jumped 30% after implementing this simple visual system.
Connecting SOAP notes to billing and insurance
Your SOAP documentation directly determines your practice's financial health. Insurance companies audit claims by comparing billing codes to treatment documentation. Mismatches trigger denials, audits, and recoupment demands.
Every CPT code billed needs specific documentation support:
-
97140 (Manual therapy)
Document specific techniques, areas treated, and time spent
-
97124 (Massage therapy)
Document medical necessity, areas, techniques, and response
-
97110 (Therapeutic exercises)
Document specific exercises, sets, reps, and client performance
The timing matters too. Bill for 60 minutes but your notes indicate 45? Claim denied. Bill for neuromuscular work but notes only mention relaxation massage? Claim denied.
A defensible billing-documentation connection looks like this:
Insurance claim: 97124 x 4 units (60 minutes) for chronic lower back pain
SOAP support:
-
S
"Lower back pain 7/10, worse with sitting, improves with movement"
-
O
"Palpation revealed hypertonicity in lumbar paraspinals L2-L5, trigger points in quadratus lumborum bilateral, applied deep tissue and neuromuscular techniques to affected areas x 60 minutes"
-
A
"Decreased muscle tension observed, client reported pain reduction to 4/10"
-
P
"Continue 2x weekly for 4 weeks, add stretching exercises"
This level of detail feels excessive until it saves you from a $20,000 recoupment demand.
Technology infrastructure and security requirements
Paper SOAP notes create physical storage nightmares. Digital systems create security nightmares. Either way, you need infrastructure that balances accessibility with protection.
For digital systems, baseline security includes:
-
Access controls
Individual logins for each staff member. Shared passwords are HIPAA violations waiting to happen. Role-based permissions—receptionists don't need full record access.
-
Encryption
At-rest encryption for stored files, in-transit encryption for any transmission. This means encrypted drives and secure connections, not just password-protected PDFs.
-
Audit trails
Every access, edit, and deletion needs tracking. Who looked at what, when, and why. Most practices discover unauthorized access only during investigations.
-
Backup systems
The 3-2-1 rule applies—three copies of data, two different storage types, one offsite. Cloud backup alone isn't enough if the vendor disappears.
Physical security gets overlooked in wellness practices. That filing cabinet with 500 client records? It needs more than a basic lock.
Consider locked room or closet for records storage, limited key distribution with tracking, visitor access restrictions, security cameras for high-value areas, and fire-resistant storage for irreplaceable documents.
A massage clinic in Phoenix had beautiful digital security—encrypted drives, secure cloud storage, perfect HIPAA compliance. Then someone broke into their office and stole the filing cabinet with three years of paper intake forms. The breach notification alone cost $8,000.
Staff training and accountability systems
The best SOAP system fails if staff don't follow it consistently. This isn't about therapists being lazy or rebellious. It's about competing priorities and unclear expectations.
New therapist orientation needs dedicated SOAP training:
-
Template walkthrough with examples
-
Practice sessions with feedback
-
Review of common documentation errors
-
Legal implications of poor documentation
-
How notes connect to billing and insurance
Don't just hand someone a template and expect compliance. Practices spend two hours on massage techniques and five minutes on documentation training. Guess which causes more business problems?
Ongoing accountability requires regular audits. Not punitive investigations—quality checks that catch problems before they become disasters. Monthly random note reviews (5-10 per therapist), quarterly documentation accuracy assessments, annual compliance training updates, and immediate feedback on documentation issues.
Create documentation champions. The therapist who writes excellent SOAP notes becomes the mentor for others. They get extra compensation for this role. Makes documentation excellence something to aspire to, not endure.
Common documentation mistakes that trigger audits
Certain documentation patterns attract regulatory attention like magnets. Avoid these red flags:
Cookie-cutter notes: Same exact wording across multiple sessions or clients. Regulators know you're not doing identical treatments every time. Variation is normal and expected.
Retroactive documentation: Writing three weeks of notes the night before an audit. Timestamps and writing patterns give this away immediately.
Impossible timelines: Documenting 15-minute breaks between clients but billing for back-to-back sessions. Math matters in audits.
Missing signatures: Unsigned notes might as well not exist from a legal perspective. Electronic signatures count if properly authenticated.
Inconsistent information: Client file says "latex allergy" but notes mention using latex gloves. These contradictions destroy credibility.
A practice in San Diego got flagged because every single SOAP note ended with "client reported feeling better." For two years. Across 400 clients. The investigator knew immediately something was wrong. The subsequent audit found massive documentation shortcuts and $43,000 in improper billing.
Building your compliance system
Creating a bulletproof SOAP notes system doesn't happen overnight, but you can build it systematically:
Phase 1: Standardization (Month 1)
Choose or create your SOAP template. Get all therapists using the same format. Establish minimum documentation standards. Train everyone on requirements.
Phase 2: Storage and Security (Month 2)
Implement secure storage systems. Create access controls and permissions. Establish backup procedures. Document security protocols.
Phase 3: Retention and Disposal (Month 3)
Build retention schedule. Create disposal procedures. Document retention policies. Train staff on requirements.
Phase 4: Integration (Months 4-6)
Connect documentation to billing. Create handoff protocols. Implement quality checks. Regular audit cycles.
This is where AI-powered operational software becomes genuinely transformative. Instead of managing paper forms, scanning documents, and manually tracking retention schedules, modern platforms handle the entire SOAP workflow automatically. Therapists complete standardized digital forms that enforce compliance requirements. The system automatically stores, encrypts, and backs up records. Retention schedules run automatically with documented disposal when appropriate.
The real value isn't just digitization—it's the operational intelligence these systems provide. They flag incomplete documentation before it becomes a compliance issue. They track patterns that might trigger audits. They ensure billing codes match documentation. They make handoffs seamless by surfacing relevant information from previous sessions.
Here's a simple workflow diagram that shows the phased implementation and ongoing audit loop.
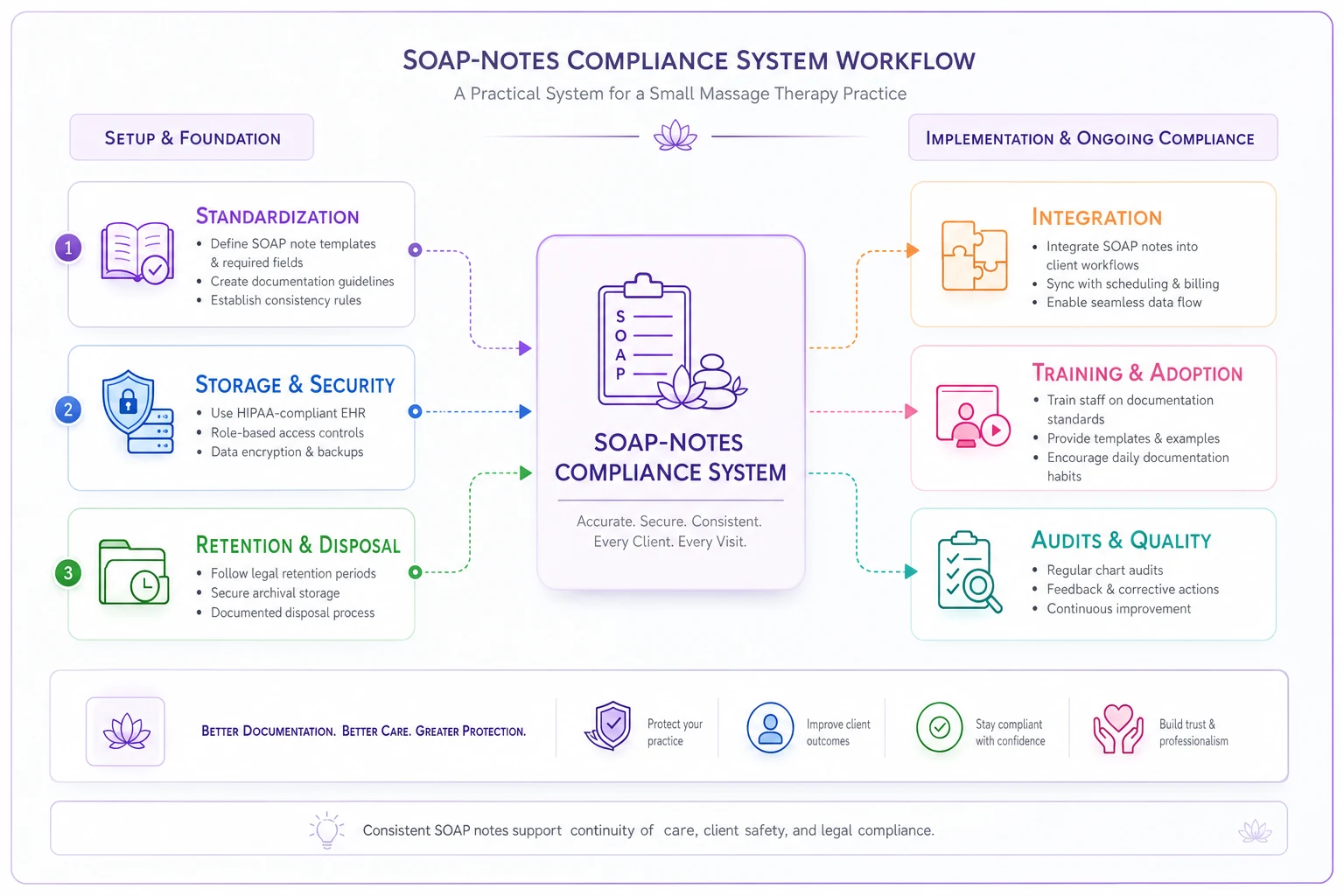
The diagram maps phase start, key actions, handoff points, and audit checkpoints.
The actual cost of poor documentation
Weak SOAP documentation costs more than just audit fines.
The operational damage spreads throughout your practice:
Weak SOAP documentation costs more than just audit fines. The operational damage spreads throughout your practice:
Ready to elevate your massage therapy business?
Join hundreds of therapists using Masthera to save time, reduce scheduling conflicts, and enhance client satisfaction.